Subscribe now to get notified about IU Jharkhand journal updates!
Tuberculosis (TB) continues to be a major public health concern in India. Though Kerala records the lowest TB prevalence in India, with just 115 cases per lakh population, it is still a public health issue in the state. In Kerala, government medical practitioners and private medical practitioners play a significant role in maintaining the state's healthcare delivery, including TB reporting and management. However, little is known about the private practitioners' knowledge regarding TB management;therefore, this study aims to assess the baseline knowledge of TB among private doctors practising in Kasargod district, Kerala. The study, using a Tuberculosis Survey among Indian Private Medical Practitioners,collected data on practitioners' awareness of TB causation, routes of transmission, risk groups, symptoms, diagnostic protocols, preventive measures, and treatment guidelines. The findings revealed knowledge gaps in critical areas such as the interpretation of diagnostic tests, understanding of latent versus active TB, awareness of drug regimens, and familiarity with national strategies like the Directly Observed Treatment Short-course (DOTS). These gaps highlight the urgent need for capacity-building initiatives and continuous medical education for private practitioners in Kerala. Strengthening their knowledge base is essential for improving TB management and supporting Kerala's goal of complete TB elimination.
Introduction
Tuberculosis (TB) is a major public health challenge in India. According to WHO, India accounts for about a quarter of the global TB burden, with 27% of (10 million) cases and 25% of the (1.6 million) deaths (Dhamnetiya et al., 2021). It is estimated that one-fourth of the annual global incidence of TB occurs in India (Dhamnetiya et al., 2021). To address the spread of the global TB epidemic within the country, there is a pressing need for the rapid implementation of an active National TB control program in India. Given that a substantial percentage of global TB patients reside in India, accelerating TB prevention measures in the country becomes a prerequisite for ending the global TB epidemic (Kruk et al., 2018).Realising the seriousness of this public health issue, the Government of India adopted several plans to eliminate TB by 2025 (Singh & Kumar, 2019). In a strict sense, TB elimination means there should be < l case of TB for a population of 10 lakh (Prasad et al., 2017). The World Health Organisation's END TB Strategy, adopted by the World Health Assembly in 2014, also aims to end the global TB epidemic with the target to reduce TB deaths by 95% and to cut new cases by 90% between 2015 and 2035, and to ensure that no family is burdened with catastrophic expense due to TB. It has set interim milestones for 2020, 2025, and 2030 (Central TB Division, Ministry of Health and Family Welfare, Government of India, 2017). However, there are challenges to achieving this goal.Local decreases in the incidence of tuberculosis in India correlate with improvements in social and economic determinants of health more than with access to quality treatment. With proper management, care and treatment, TB patients can be cured and the battle against TB can be won.
In India, the private sector plays a significant role in TB diagnosis and treatment, accounting for 70% of the cases. Despite the lack of uniform quality and standard protocols for TB care programs in the private sector, private practitioners contribute significantly to TB care, even without standardised protocols or Standardised Patients (SPs) for diagnosis and treatment (Hazarika, 2011; Rakesh et al., 2022). The Indian government has recognised the importance of private healthcare providers in delivering curative services to the majority of the population in India and has tried to include these providers in the national TB control efforts (Arsenault et al., 2019).
While India continues to struggle with managing tuberculosis (TB), Kerala has made notable progress, particularly in reducing drug-resistant TB transmission, through initiatives like the Kerala Tuberculosis Elimination Mission, a People's movement against TB supported by local government institutions. However, most existing studies on TB in India have predominantly focused on government programmes and the knowledge, practices, and cha11enges within the public health sector. The role of private practitioners, who form a critical component of Kerala's healthcare system and often serve as the first point of contact for patients, remains largely unexplored. This gap highlights the need to examine the awareness, diagnostic practices, and treatment approaches of private practitioners in Kerala, as their involvement is essential for strengthening TB control and achieving elimination goals. This paper aims to address this research gap.
Methodology
This study employed a descriptive cross-sectional survey design to assess the knowledge of private doctors in Kasargod regarding the standard protocols for TB care programs. The study population consisted of 30 private medical practitioners actively practising in the district with a minimum of five years' experience. The respondents were recruited from the General Practitioners, Pulmonologists, General Physicians, Paediatricians and Infectious Disease Specialists from the private hospitals in Kasaragod, including clinics, secondary hospitals, speciality hospitals, super speciality hospitals and nursing homes. A structured questionnaire, which was developed based on the guidelines and recommendations of the World Health Organisation (2025) and the National Tuberculosis Elimination Programme (NTEP) of India, was administered (Central TB Division, Ministry of Health & Family Welfare, 2024).The study framed a survey model based on the knowledge, attitudes, and practices (KAP) survey model, which is found to be the best for assessing the awareness about TB. This is a representative study of a specific population to assess what is known, believed, and done in relation to TB(Craciun et al., 2023).The questionnaire was divided into multiple sections: basic biomedical knowledge, clinical features and symptom recognition, diagnosis and screening practices, infection control and prevention measures, treatment and management knowledge, and epidemiological awareness specific to India.Data were collected through direct interviews and self-administered responses toensure that all respondents provided complete answers. The questionnaire included multiple-choice questions and closed-ended items to capture precise information about the respondent's understanding of TB etiology, transmission, risk factors, latent versus active disease, hallmark symptoms, diagnostic protocols, screening tests, treatment regimens, drug resistance, infection control measures, referral practices, and national TB program strategies.Descriptive statistical analysis was conducted to summarise the responses. It used SPSS to calculatefrequencies and percentages for each question and to identify knowledge strengths and gaps. The analysis focused on identifying correct versus incorrect responses, common misconceptions and areas of uncertainty among respondents.
Population and Demography
The demographic profile of the respondents reveals a diverse and experienced group of medical professionals. Their ages ranged from 27 to 90 years, with most falling between 30 and 60 years, and the majority of the respondents were male,with 63.3% of the population compared to the female populationwith 36.7%. Most respondents were from Kerala (76.7%), followed by Karnataka (20%) and Tamil Nadu (3.3%). Professionally, general practitioners work as consultants, forming the largest group of respondents with 26.9% of the respondents. Other professional groups included Pulmonologists,General Physicians andPaediatricians. Years of experience varied widely, from 5 to 48 years in medical practice and 5 to 41 years in general practice, with many having more than 15 years of experience, reflecting a well-seasoned medical sample. The number of TB or latent TB cases diagnosed over the last three years ranged from none to as many as 200. All respondents who specified location were based in Kasargod, and their workplaces included clinics (63.6%)and other institutions such as hospitals, nursing homes, and multi-speciality centres(36.4%). While 72.4% had experience managing TB patients, 27.6% had not, and only half had attended a lecture, seminar, or workshop on TB in the past year, indicating both awareness and the need for continued training.
Table 1
Demographic profile of the respondents
|
Demographic Factor |
Categories |
% |
|
Age Group |
20-39 yrs (30%), 40-59 yrs (53.3%), 60+ yrs (16.6%) |
100 |
|
Gender |
Male (63.3%), Female (36.7%) |
100 |
|
State |
Kerala (76.7%), Karnataka (20%), Tamil Nadu (3.3%) |
100 |
|
Designation |
Consultants (26.9%), Paediatricians (19.2%), Others (53.9%) |
100 |
|
Experience |
<10 yrs (30%), 10-19 yrs (20%), 20+ yrs (50%) |
100 |
|
Worked with TB patients Yes (72.4%), No (27.6%) |
100 |
|
|
Institution TypeClinic (63.6%), Others (36.4%) |
100 |
|
|
Attended TB Seminar Yes (50%), No (50%) |
100 |
Findings
The comprehensive analysis of the knowledge and awareness of TB-related information among the private doctors in Kasargod revealed significant conclusions. The assessment focused on several key domains such as basic biomedical knowledge, clinical features and symptom recognition, diagnosis and screening practices, infection control and prevention measures, treatment and management protocols, and India-specific epidemiological awareness.In the domain of biomedical knowledge, the study analysed respondents' understanding of TB etiology, transmission routes, high-risk groups, and the distinction between latent and active TB. In the domain of clinical knowledge, the study evaluated theawareness of the key symptoms of pulmonary TB. In the domain of diagnostic and screening knowledge, the study assessed familiarity with standard tests, sample collection and interpretation of results. The study assessed the treatment and management knowledge through the analysis of the responses on the first-line anti-TB drugs, duration of therapy, MDR-TB, DOTS, and referral practices. The study also assessed the epidemiological knowledge on TB incidence and mortality rates in India. This structured analysis provides a detailed overview of strengths, misconceptions, and gaps in private doctors' TB-related knowledge, informing potential areas for targeted interventions and continuing medical education.
Basic Biomedical Knowledge
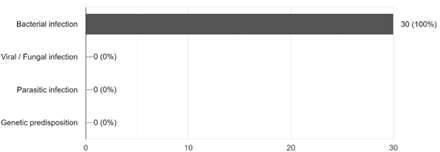
The analysis of the responses on the cause of tuberculosis, all the private doctors correctly identified it as a bacterial infection. None of the respondents selected viral/fungal infection, parasitic infection, or genetic predisposition as possible causes. This suggests that the respondents possess aclear and accurate understanding of the fundamental etiology of TB, namely infection with Mycobacterium tuberculosis. The absence of misconceptions at this basic level indicates strong biomedical knowledge among the doctors surveyed.
Figure 1
Distribution of the causes of TB among the respondents
The analysis of the responses on the most common transmission route of tuberculosis, all respondents correctly identified airborne droplets as the mode of spread. None of the respondents selected direct skin-to-skin contact, contaminated water/food, or sexual contact. This uniform response reflects ahigh level of awareness about TB's primary transmission mechanism. It also indicates that misconceptions about non-airborne modes, such as food, water, or sexual transmission, are absent among the respondents, which is critical for accurate patient education and infection control practices.
When asked who is at the highest risk of developing tuberculosis, the vast majority of respondents (93.3%) correctly identified people with weakened immune systems, such as those living with HIV/AIDS, as the most vulnerable group. A very small proportion of respondents incorrectly attributed a higher risk to young adults (3.3%) and individuals with strong immunity (3.3%). Notably, none of the selected elderly individuals over 65 were considered to be at higher risk. These finding highlights that while most doctors demonstrated sound knowledge of the key risk group, a minor fraction (6.6%) hold misconceptions about TB susceptibility. Such misconceptions, although limited, could potentially influence clinical decision-making and patient counselling, particularly in identifying and prioritising vulnerable populations for screening and preventive interventions.
The majority of respondents (86.7%) correctly recognised that latent TB is not contagious, reflecting a sound understanding of the disease's clinical course. A smaller proportion (13.3%) answered that it is contagious only during the active stage, which is also partially correct since TB becomes transmissible only when active, not latent. Importantly, none of the doctors expressed misconceptions that latent TB itself is contagious or that its contagiousness depends
on individual variability. This finding indicates that private doctors in Kasargod generally possess accurate knowledge about the non-contagious nature of latent TB. However, a small subset frames the answer in terms of active-stage contagion rather than absolute non-contagiousness. This suggests room for improved conceptual clarity, but no major misconceptions are present.
All respondents correctly identified that active TB is contagious, demonstrating complete and accurate knowledge of this fundamental aspect of TB transmission. This unanimity suggests that private doctors in Kasargod are well aware of the public health risks associated with untreated active TB and, by extension, the importance of timely diagnosis, isolation, and treatment. The responses clearly show that the majority of respondents correctly identified infection through airborne transmission, specifically when a person inhales droplets released by someone with active TB during coughing, sneezing, or even talking. This indicates astrong level of awareness about the primary route of TB infection among respondents. Only a small number of responses pointed toward incorrect modes of infection, such as through food, water, or physical contact, suggesting that some misconceptions persist about TB spread. These misperceptions, while limited, highlight the importance of continuing health education and awareness programs to ensure accurate understanding. The conclusions revealed that most respondents have a sound grasp of TB's infectious nature, but targeted clarification is needed to correct the few remaining misunderstandings.
Most respondents identified high-risk groups of TB accurately, such as individuals with weakened immune systems (including those with HIV/AIDS, diabetes, or malnutrition), people living in overcrowded or poorly ventilated environments, and those from economically disadvantaged backgrounds with limited access to healthcare. A smaller proportion of responses reflected less accurate perceptions, such as attributing TB risk to factors like age alone or lifestyle habits, showing that some misconceptions remain about risk determinants.
The analysis of the responses on whether a person infected with TB can go through life without developing the disease indicates that 24.1% of respondents correctly answered "Yes", recognising that individuals with latent TB infection may never develop active disease. The majority ofrespondents either answered "No" or were ''Not sure," suggesting limited awareness or uncertainty about the concept of latent TB. This highlights a knowledge gap regarding
the natural history of TB infection, which is important for understanding risk, monitoring, and preventive treatment strategies.
Knowledge on Clinical Features and Symptoms
The analysis of the responses on the hallmark symptoms of TB, such as cough, chest pain, weight loss, fever, night sweats, and hemoptysis, revealed that the majority of respondents were aware of the symptoms of TB. At the same time, a smaller number of doctors mistakenly associated TB with non-specific or unrelated symptoms such as abdominal pain, joint pain, headache, nausea, and skin rash.This pattern suggests that while knowledge of classical pulmonary TB symptoms is strong among private doctors in Kasargod, some misconceptions remain, pointing to occasional overgeneralisation of TB symptomatology. Such misconceptions may affect differential diagnosis and could lead to either over-suspicion or under-recognition of TB in atypical cases.
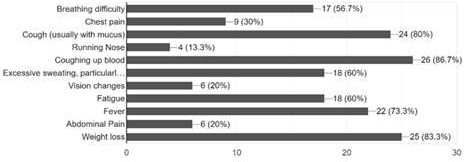
The analysis of the responses on the main symptoms of pulmonary TB revealed, as shown in figure 1, that most respondents correctly identified the hallmark signs of the disease, with fever (86.7%), weight loss (83.3%), cough with mucus (80%), excessive sweating, particularly at night (73.3%), coughing up blood (60%), fatigue (60%), breathing difficulty (56.7%),and chest pain (56.7%) being the most frequently recognised. In contrast, fewer respondents associated TB with a running nose (13.3%), vision changes (20%), orabdominal pain (20%), which are not typically characteristic of pulmonary TB. This indicates a strong awareness of core TB symptoms. However, the inclusion of unrelated symptoms highlights the persistence of misconceptions, underlining the need for targeted health education to improve public understanding of the disease.
Figure 2
Distribution of the knowledge regarding the symptoms of pulmonary TB
Diagnosis and Screening Knowledge
The majority of respondents (86.7%) correctly recognised sputum smear microscopy as the standard diagnostic test for TB, consistent with both WHOand National TB Elimination Programme (NTEP)guidelines in India. A small fraction, however, incorrectly selected TST and IGRA, which are screening tools rather than confirmatory diagnostic tests. Importantly, no respondents chose irrelevant options such as Helicobacter pylori testing. This suggests that while most private doctors in Kasargod have accurate knowledge of TB diagnosis, a minority confuse screening tools with diagnostic tools, which could impact clinical decision-making and delay appropriate treatment initiation.
The analysis of the responses indicated that respondents were aware of multiple screening methods for TB. The most commonly identified tests were chest X-rays and sputum smear microscopy, both recognised as frontline tools for detecting TB infection. A smaller number of respondents mentioned the Mantoux tuberculin skin test and blood tests such as the interferon-gamma release assay (IGRA), reflecting knowledge of more advanced screening methods. The distribution suggests that while the majority had a good understanding of the standard diagnostic approaches, awareness ofless commonly used or advanced screening tests was relatively limited. The analysis of the responses showed that most respondents correctly identified that two to three sputum samplesare required for accurate TB diagnosis, aligning with standard medical guidelines. A noticeable proportion, however, either underestimated by indicating only one sample or was uncertain, reflecting partial knowledge. This suggests that while the majority of respondents are aware of the need for multiple samples to ensure reliability in TB detection,
there are still knowledge gaps regarding the exact number required.
The analysis of the responses on the first examination/test for a patient suspected of pulmonary TBshowed that the majority of respondents correctly identified sputum smear microscopy/culture (70%) as the primary diagnostic test; this reflects good awareness of the standard diagnostic approach. A smaller proportion selected chest X-ray (36.7%) and the Mantoux test (30%), which can support diagnosis but are not definitive on their own. Notably, no respondent chose irrelevant options such as CRA test, blood culture, or responded with "I am not sure," indicating that the group had a relatively clear understanding of appropriate TB diagnostic protocols. The responses suggest a strong grasp of sputum testing as the gold standard. However,some respondents' reliance on chest X-rays and Mantoux tests points to partial misconceptions about confirmatory versus supportive diagnostic tools.
The assessmentof responses on whether a negative chest X-ray excludes TB disease indicated that most respondents answered "No" (79.3%), correctly recognising that TB can still be present despite a standard X-ray, especially in cases of early infection, extrapulmonary TB, or latent TB. A smaller proportion responded "Yes"(13.8%); this reflects a misconception that a clear X-ray rules out TB entirely. Additionally, 6.9%were "not sure," suggesting some uncertainty. The results highlight that while the majority of respondents demonstrate accurate knowledge of the limitations of chest X-rays in TB diagnosis, a minority still hold incorrect assumptions or lack confidence, which may impact timely and accurate case detection.
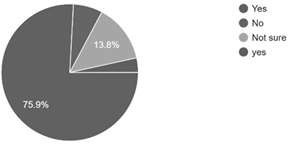
The assessmentof responses on whether a patient with a positive IGRA test should be referred to a specialist for further examination for active or latent TBindicates that only a small proportion of respondents (13.8%) correctly answered "Yes",recognising the need for further evaluation by a specialist. The majority of respondents either answered "No" or were "Not sure," suggesting limited awareness or uncertainty about the appropriate follow-up for a positive IGRA result. This highlights a significantknowledge gap regarding the interpretation of screening tests and referral protocols, which could impact timely diagnosis and management of both latent and active TB cases in clinical practice.
Figure 3
Distribution of responses on whether a patient with a positive IGRA test should be referred to a specialist
The examination responses on whether a positive Mantoux test indicates a defmite TB infection showed that the majority of respondents correctly answered "No", recognising that a positive result indicates exposure to Mycobacterium tuberculosis but does not confirm active disease. A smaller proportion either answered "Yes" or were ''Not sure,"reflecting misconceptions about the diagnostic value of the Mantoux test. These results suggest that while most private doctors in Kasargod understand the screening versus diagnostic nature of the Mantoux test, a few still require clarification to avoid misinterpretation in clinical practice.
Infection Control andPrevention Knowledge
The responses regarding infection control and prevention proceduresreveal a mixed understanding among respondents. A portion of respondents believed that a surgical mask is effective in preventing TB transmission. In contrast, others correctly recognised that surgical masks alone are not sufficient for protection against TB, as TB spreads through airborne particles that require respirators like N95 masks for effective prevention. This indicates that while some awareness exists regarding protective measures, there remains confusion between general infection control masks and specialised respiratory protection needed for TB. At the same time, the responses demonstrate a strong awareness of the protective role of N95 masksagainst TB. The majority of respondents identified that N95 masks are effective, though some variation existed in the perception of their degree of effectiveness. While most respondents agreed that N95 masks provide reliable protection, a smaller proportion believed that they offer only partial protection or that their use is mainly relevant for health care workers. Very few, if any, considered them to be completely ineffective. This suggests that respondents generally recognise the importance of N95 masks in preventing TB transmission. However, there is still some misunderstanding about their universal applicability and the contexts in which they should be used.
The analysis of the responses showed thatthe majority of respondents were aware of environmental control strategies, with a significant portion correctly identifying measures such as proper ventilation, sunlight exposure and air circulation as effective in reducing TB transmission. Most respondents chose the correct options; this highlights a strong understanding that TB bacteria thrive in enclosed, poorly ventilated spaces and can be reduced through adequate airflow and natural light. However, a smaller fraction of respondents either selected incorrect or less relevant measures, which suggests that while awareness of environmental control is relatively high, there remains aneed for reinforcing knowledgeon how these interventions should be practically implemented,such as the use of exhaust fans, cross-ventilation, and UV germicidal irradiation in high-risk areas.
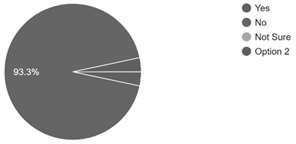
The examination of the responses to whether the previous BCG vaccine ensures 100% protection against TB diseaserevealed that the majority of respondents answered
"No"(86.7%), correctly understanding that while the BCG vaccme offers some protection, especially in children against severe forms of TB, it does not guarantee complete immunity. A sma11 fraction responded "Yes" (6.7%);this reflects the misconception that BCG provides absolute protection.Another 6.7% were "Not sure" about the effectiveness of the BCG; this indicates uncertainty about the vaccine's effectiveness. These conclusions suggest that most respondents have a sound understanding of the limitations of BCG vaccination. However, a small group still requires clarification regarding its partial and age-dependent protective role.
Figure 4
Respondents' perspective regarding the BCG vaccine
Treatment andManagement Knowledge
The assessmentof the responses on MDR TB (Multi-Drug-Resistant Tuberculosis)indicated that the majority of respondents correctly identified it as a form of TB resistant to at least two of the most powerful first-line anti-TB drugs, isoniazid and rifampicin. A small proportion of respondents selected incorrect definitions; this shows themisunderstandings about drug resistance in TB. The results suggest that while most private doctors in Kasargod have a good grasp of MDR TB, there remains a need for further education to ensure precise knowledge of drug resistance mechanisms and implications for treatment.
The analysis of the responses on the duration for which anti-TB drugs are usually prescribed for newly diagnosed pulmonary TBindicates that the majority ofrespondents (73.3%) correctly reported a treatment duration of 6 to 9 months, consistent with the National Tuberculosis Elimination Programme (NTEP) guidelines for first-line therapy. A smaller proportion selected 4 to 6 months (13.3%)or 2 to 4 months (6.7%), reflecting partial knowledge or misconceptions regarding the standard regimen. Additionally, 6.7% of respondents indicated "I do not know," suggesting uncertainty among a few practitioners. The findings demonstrate that most private doctors in Kasargod are aware of the recommended treatment duration, though some knowledge gaps remain that could affect adherence and treatment outcomes.
The analysis of the responses on knowledge of standard anti-TB medications in Indiaindicates that the majority of respondents correctly identified the first-line anti-TB drugs, includinglsoniazid, Rifampicin, Pyrazinamide, and Ethambutol, as part of the standard treatment regimen.This demonstrates a strong understanding of the essential pharmacological components of TB therapy among private doctors in Kasargod. A small proportion of respondents, however, either selected incorrect options or indicated uncertainty, suggesting minor gaps in knowledge regarding complete treatment protocols. Overall, the results reflect that most respondents are aware of the core medications used in the National Tuberculosis Elimination Programme (NTEP), which is crucial for ensuring effective patient management and adherence to treatment guidelines.
The analysis of the responses on the primary national treatment strategy of the National Tuberculosis Control Programme (NTEP) in lndiaindicated that the majority of respondents correctly identified the Directly Observed Treatment Short-course (DOTS) strategy as the cornerstone of TB management. A smaller number of respondents selected options such as preventive therapy, early detection and diagnosis, or use of GeneXpert MTB/RIF technology, reflecting partial understanding of NTEP components versus the core treatment strategy. Overall, these results suggest that while most private doctors in Kasargod are aware of the primary national TB treatment approach, there is someconfusion regarding the distinction between the overall program elements and the central DOTS strategy .It highlights the need for reinforcement of program-specific knowledge.
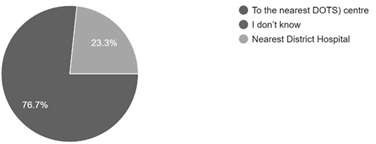
The analysis of the responses on referral practices for a patient with confirmed, previously untreated TBindicates that only 23.3% of respondents correctly identified referral to the nearest DOTS centre, which is the recommended pathway under the National TB Elimination Programme (NTEP). The remainder either chose the nearest district hospitalor "I do not know," reflecting uncertainty or lack of clarity about the official referral protocol. This suggests a significant gap in knowledge regarding appropriate patient referral, which could delay treatment initiation and impact TB control efforts in the private healthcare sector.
Figure 5
Awareness of DOTS Centre
The analysis of the responses on DOT (Directly Observed Therapy)indicates that the majority of respondents correctly identified it as Directly Observed Therapy, the internationally recommended strategy in which a healthcare provider or trained worker supervises the patient taking their TB medication to ensure adherence. A smaller proportion of respondents selected incorrect interpretations, such as Distribution of Tablets, Daily Oral Treatment, or Doctor's Oversight Technique, reflecting some confusion about the specific purpose and methodology of DOT. Overall, these results suggest that while most private doctors in Kasargod are familiar with the concept of DOT, a few misunderstand the precise implementation and rationale, highlighting the need for targeted reinforcement of treatment adherence strategies.
Epidemiological Knowledge
The analysis of the responses on the annual TB mortality in Indiaindicated that only a small proportion of respondents correctly estimated the number of TB-related deaths, with 10.7% selecting the accurate figure of 320,000 deaths per year. A larger proportion chose lower estimates, such as 224,000 (17.9%) and 220,000 (25%); this reflectsunderestimation of the disease burden. This suggests that while private doctors are generally knowledgeable about TB diagnosis and treatment, there is limited awareness of the actual national mortality statistics, which could affect their perception of TB's public health impact and urgency in clinical practice.
The analysis of the responses on the annual number of TB diagnoses in India (27 responses) shows that respondents' estimates varied, reflecting limited awareness of the accurate scale of TB incidence. While the actual number is over 2 million new cases annually, respondents selected a range of options from 1 million to 4 million, indicating both underestimation and overestimation of the TB burden. This highlights a knowledge gap regarding the epidemiological magnitude of TB in India, which is important for understanding the public health challenge and prioritising timely diagnosis, reporting, and treatment interventions.
Discussion
The present study examined the knowledge of private doctors in Kasargod regarding tuberculosis (TB) with reference to the recommendations of the World Health Organisation (2025) and the National Tuberculosis Elimination Programme (NTEP) of India. The analysis focused on exploring various domains of TB-related knowledge among private medical practitioners, such as biomedical understanding, clinical features, diagnostic and screening practices, infection control, treatment and management and epidemiological awareness specific to India. The study revealed a strong foundational knowledge among respondents, though notable gaps persist in specific areas that may influence clinical practice and public health outcomes.
The respondents demonstrated excellent understanding of TB etiology and transmission. Previous research has shown that biomedical understanding of TB among medical practitioners is a key factor in determining the elimination of TB (Churchyard et al., 2017; Leo et al., 2024).All respondents correctly identified TB as a bacterial infection and recognisedairborne droplets as the primary route of transmission. It indicates strong biomedical literacy and the absence of misconceptions at a basic level. Most doctors (93.3%) correctly identified immunocompromised individuals, such as those with HIV/AIDS, as being at the highest risk, reflecting awareness of key vulnerability factors. However, a small fraction (6.6%) held misconceptions about risk groups. Importantly, the majority understood that latent TB is non-contagious (86.7%) while recognising that active TB is infectious, highlighting an accurate grasp of TB's clinical course and transmission dynamics. However, only 24.1% acknowledged that latent TB may remain asymptomatic throughout life, indicating a need for improved understanding of disease progression and preventive strategies.
Respondents showed strong recognition of hallmark TB symptoms. Core signs such as cough, fever, weight loss, night sweats, hemoptysis, chest pain, fatigue, and breathing difficultywere widely acknowledged, demonstrating a sound grasp of pulmonary TB presentation. However, some respondents erroneously associated non-specific or unrelated symptoms, such as abdominal pain, joint pain, nausea, headache, or skin rash, suggesting occasional overgeneralization of symptomatology. These misconceptions could affect differential diagnosis and potentially lead to misidentification of TB in atypical presentations.
Early TB diagnosis is critical for global health since it prevents TB transmission; however, it requires the proper and advanced knowledge of diagnostic protocols among the practitioners (Dong et al., 2022; Filardo et al., 2022; Bartolomeu-Gorn;:alves, 2024).Knowledge of diagnostic protocols was generally good. A majority (86.7%) correctly identified sputum smear microscopy as the gold standard, while most also recognisedchest X-ray, Mantoux test, and IGRA as supportive or screening tools. Awareness of the need for two to three sputum samples was every day, though some respondents underestimated this requirement. Regarding the first test to perform in suspected pulmonary TB, most selected sputum smear microscopy/culture (70%), while smaller fractions chose chest X-ray or Mantoux test, indicating partial reliance on supportive rather than definitive diagnostic tools. Notably, only 13.8% correctly indicated that patients with a positive IGRA test should be referred to a specialist, revealing a substantial gap in referral and follow-up knowledge.
Respondents demonstrated mixed understanding of protective measures. While the majority correctly identified N95 masks as effective and recognised environmental controls such as ventilation and airflow, some believed surgical masks were sufficient, indicating confusion regarding appropriate respiratory protection. Additionally, most respondents correctly noted that the BCG vaccine does not provide complete protection (86.7%), reflecting an accurate understanding of its limitations, though a few still believed it offered complete immunity.
The selection of an appropriate drug regimen is essential for the timely and pattern-based treatment of TB. It is significant for the medical practitioners in India to recognise the different available drugs and regimens currently in use for TB disease (Gill et al., 2022). It has been found that the respondents' knowledge of TB drugs and treatment protocols was strong in core areas. Most respondents correctly identified first-line drugs such as Isoniazid, Rifampicin, Pyrazinamide, Ethambutol, and the DOTS strategy as central to NTEP. They also accurately described MDR TB as resistance to at least isoniazid and rifampicin and reported the correct treatment duration of 6-9 months for newly diagnosed patients (73.3%). However, referral knowledge was limited, with only 23.3% correctly identifying the nearest DOTS centre as the appropriate point for treatment initiation. Knowledge of DOT itself was strong, but minor misconceptions about its implementation highlight the need for reinforcement of adherence protocols.
A significant knowledge gap emerged in respondents' understanding of TB incidence and mortality in India. Only 10.7% correctly estimated annual TB deaths (320,000), while estimates of diagnosed cases varied widely, reflecting underestimation or overestimation. This suggests that while clinical and biomedical knowledge is high, awareness of national epidemiological data is limited, which may influence perceptions of TB as a public health priority.
Implications
The findings suggest that private doctors in Kasargod possess strong biomedical knowledge and familiarity with core clinical, diagnostic, and treatment principles of TB. However, gaps in understanding latent TB, referral protocols, the interpretation of screening tests, infection control nuances, and national epidemiology point to areas requiring targeted continuing medical education. Strengthening these domains could improve early diagnosis, appropriate referral, adherence to treatment protocols and public health interventions, ultimately contributing to more effective TB control in the private healthcare sector.
Recommendations
Based on the key findings derived from this analysis, the study proposes a few recommendations that can enhance TB knowledge, clinical practices, and control efforts among private doctors in the Indian context. There is a need to strengthen continuing medical education (CME) programs focusing on latent TB, screening test interpretation, referral protocols, and national TB epidemiology to reinforce the public health significance of TB in India. Diagnostic and screening knowledge should be improved, with an emphasis on the distinction between confirmatory tests, such as sputum smear microscopy and supportive tools, like Mantoux and chest X-ray, as well as the importance of collecting multiple sputum samples for accuracy. Infection control awareness must be enhanced through training on the appropriate use of personal protective equipment, particularly N95 respirators, and environmental measures such as ventilation and sunlight exposure. Doctors' understanding of TB treatment and management should be reinforced in the domains of the first-line anti-TB drugs, treatment duration, MDR TB management and adherence to Directly Observed Therapy (DOTS). Referral and follow-up procedures need clarification, ensuring patients are directed to NTEP-approved DOTS centres, supported by simple referral guidelines or flowcharts. Awareness of social and medical risk factors should be promoted to encourage risk-based screening of vulnerable populations. Additiona11y, strengthening public-private co11aboration, providing access to training resources and program updates, and encouraging the use of digital tools for diagnosis, treatment, and reporting can ensure adherence to national TB guidelines. Addressing these knowledge gaps can improve infection control, standardise patient care, and integrate private practitioners effectively into India's TB elimination efforts.
Conclusion
This study highlights that while private medical practitioners in Kasargod possess a strong foundational understanding of tuberculosis etiology, transmission, and key clinical features, important gaps remain in their knowledge of diagnostic interpretation, latent versus active TB, treatment duration, drug resistance, and referral protocols. Misconceptions regarding symptomatology, diagnostic tools, and national program strategies such as DOTS and referral to designated centres indicate areas requiring targeted capacity-building. Strengthening the knowledge base of private practitioners through continuous medical education, structured training, and closer integration with the National Tuberculosis Elimination Programme (NTEP) is crucial. Addressing these gaps will not only improve the quality of TB care in the private sector but also significantly contribute to India's goal of eliminating TB.
References
References