Subscribe now to get notified about IU Jharkhand journal updates!
In the present paper a comparative study based on the data of National Family Health Survey of Bihar and Jharkhand has been attempted. Maternal health involves number of components like health of a woman during pregnancy, childbirth, and postpartum care. Its successful implementation is quite complex in nature. State of Jharkhand has witnessed major changes since its formation. Variations are found in government expenditure on health in these states. Expenditure on health and family welfare in Bihar was 15898 crores (2022-23 BE) and that in Jharkhand was 5630 crores (2022-23 BE). Similar variations are also found in maternal and child health status in the two states. MMR in Bihar is found to be 149 (SRS 2016-18), it is 71 in Jharkhand (SRS 2016-18). Similarly in child health also the performance of Jharkhand is better than that of Bihar. Further both Bihar and Jharkhand are recognised under Empowered Action Group. Government responsibility henceforth increases and a careful examination about the performance of these states in maternal and child health indicator reflects that more expenditure and planning is required to achieve desired goals in this area.
Health and education are important aspects of human development. As defined by World Health Organisation (WHO), health is a complete physical, mental and social well-being of an individual, and not merely the absence of disease or infirmity. Further reproductive health is defined as the reproductive process, functions and system at all stages of life. One aspect of reproductive health can be linked to access of safe methods of birth control, contraception and other measures related to reproductive health of both male and females. Reproductive health problems are a major source of health problems faced by a female.
Indian being the second most populated nation of the world, its health status can play an important role in shaping global health conditions. Since in the initial stages the concepts of human development and later the concept of millennium development goals gained momentum in India, government focus on both health and education has increased. The concepts of education and health are mutually interdependent as such it could be concluded that improvement in one can lead to improvement in other. The concept of public health is multi-dimensional and it includes matters related to health facilities provided by government, cleanliness and waste-disposal issues along with providing health education (Monica Das Gupta, 2005). The outreach of private health facilities is limited in the nation. Government is entitled of the responsibility of providing both qualitative and quantitative health care facilities to the masses. Among other elements of public health, maternal and child health are important ones. Maternal health basically refers to health of a mother during pregnancy, child birth and postpartum care. Similarly, child health is concerned with infant and child mortalities, immunization, and prevalence of diseases.
Health is an important concern for both Bihar and Jharkhand. Public health facilities in these states have been lacking both in terms of quantity and quality. After the split of Bihar into Bihar and Jharkhand, both these states have witnessed many important economic and social changes. Growth rate of Bihar has been quite impressive in recent years with the state having a current GSDP figures in double digit (10.3% at constant prices in 2016-17). The state of Jharkhand has also shown impressive growth patterns (6.7% at constant prices in 2016-17). These development indicators must be reflected in performance of health indicators for these states. With this background, the present study focuses on analysing maternal and child health status of Bihar and Jharkhand. A review of government budget is also attempted to analyse expenditure pattern of the government in general and on health sector in particular. These states are also under Empowered Action Groups (EAG), so a comparison with other EAG states is also attempted later in order to have a comparative discussion.
Review of Literature
Health issues have always been a matter of concern for researchers all over the world. India has become a hub of global health research because of its huge population which plays an important part in shaping global health indicators. Also major concern of the government lies in reducing health inequalities prevalent in the country (Saikia & Kulkarni, 2016).
There exist connections between multiple vulnerabilities and the utilisation of maternal and child health care (MCH) services. Bivariate analysis and binomial-logistic regression analysis were used to examine the multiple vulnerabilities on utilising MCH services across three dimensions of vulnerabilities, such as education, wealth and caste. A multi-sectoral approach is required to deal with the issues of low access and underutilisation of MCH services (Mishra PS, 2023)
The whole idea of motherhood is generally considered very satisfying and full of emotions. The case is however, different for developed and developing countries. In developing nations it is generally associated with ill-health, mal-nourishment which may even lead to death (Dehury & Samal, 2016). The concept of public health is different from medical facilities as public health basically relates with government’s effort in reducing the masses exposure to diseases (Monica DasGupta, 2005). Public health facilities are financed by government more often than not because market has little to do in this case. This increases the responsibility of state in improving health conditions of masses. This is clearly observed in a study done in Odisha. (Suman Chakrabarti, 2021) aimed at longitudinally examine whether, and to what extent, initiation of the Mamata scheme aligned with changes in health and nutrition outcomes in Odisha, relative to other states in India. Taken together, the results suggested that the Mamata scheme may have provided with improved maternal and child health outcomes in Odisha. Also it has been observed that EAG states have lagged behind in controlling population growth to manageable levels. Government can improve the situation by enhancing the delivery, uptake and utilization of maternal and child health services (Shreyasi Roy, 2020)
Studies have been carried out across the nation to assess utilisation of maternal health care services. One such study has pointed out towards religion aspect. (Shama Firdaush, 2018) studied about the assess of health status of Muslim and Hindu women across states of India. Looking at the condition of the states individually, found that states like Kerala, Uttarakhand had the higher proportion of Hindu women whereas Assam, Jammu and Kashmir, Rajasthan had the higher percentage of Muslim women having better health facilities. In contrary were the states like Andhra Pradesh, Jharkhand and others where the health status of Hindu as well as Muslim women was found worse than others. Utilisation of maternal health care services also affects status of child health. (Susmita Dasgupta, 2019) employed logistic regression models that linked the probabilities of child wasting and maternal anaemia. They initially explored the spatial structure of the residuals using estimated state effects, which suggested spatial variation.
In India, over the years public health in general and maternal and child health in particular has been on government’s priority. Maternal and Child Health (MCH) was first initiated in India during early 1900s. In 1946, Bhore committee recommended the integration of MCH in general health facilities. Gradually the horizons of Maternal Health services expanded and health care facilities increased (Singh, 1997). Currently National Health Mission is focusing on improving maternal and child health status in the nation.
Data and Methodology
This is descriptive study wherein data from various rounds of NFHS (NFHS -1 to NFHS -5) have been used. Quantitative techniques like percentage and proportion have been used to analyse the data. For comprehensive understanding, graphs and pie-charts have been used.
Findings and Analysis
Fertility and Family Planning
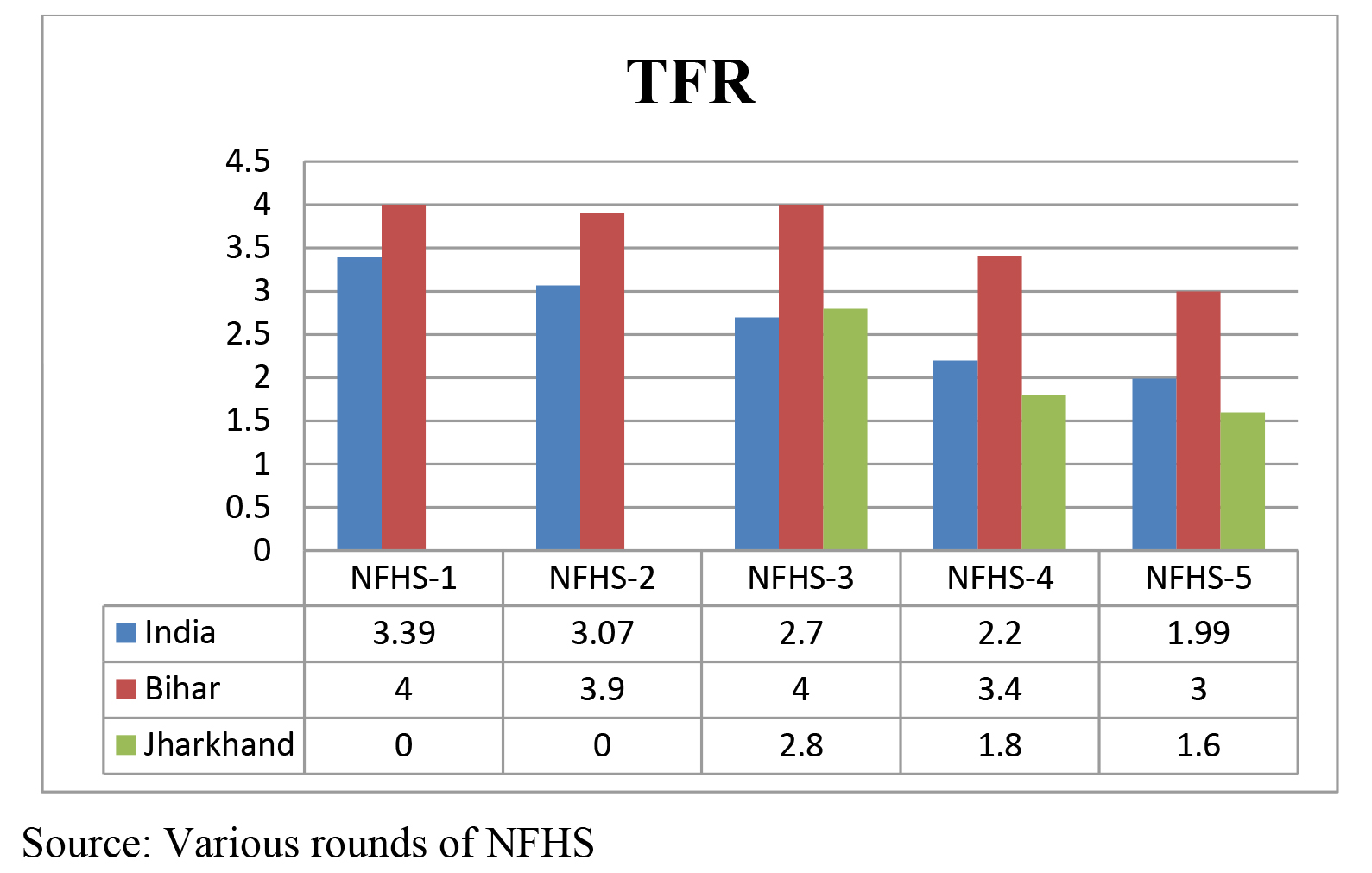
Total Fertility Rate: Fertility clearly defines reproductive capacity of a woman. More precisely it is a measure of number of children a woman will have in her entire reproductive span provided she is subject to current age-specific fertility rate. The TFR figures for Bihar and Jharkhand show different patterns. The TFR figures for Jharkhand have reached below the replacement level (1.6). However, Bihar still has a TFR of 3.0 indicating that an average woman in the state has around 3 children in her entire reproductive span. All-India figures have reached replacement level of 1.9. A comparison with NFHS-3 data reveals that Jharkhand has shown a considerable progress is controlling fertility rates in the state. In Bihar also, TFR figures have reduced from 4(2005-06) to 3.0 (2019-20) although the pace of decline is slow. This can be correlated with the literacy level of females in the state. Literacy level of females in Bihar is below 50% and hence fertility levels are still high in the state. This can further be associated with the use of family planning methods by couples. The analysis is presented in preceding paragraphs.
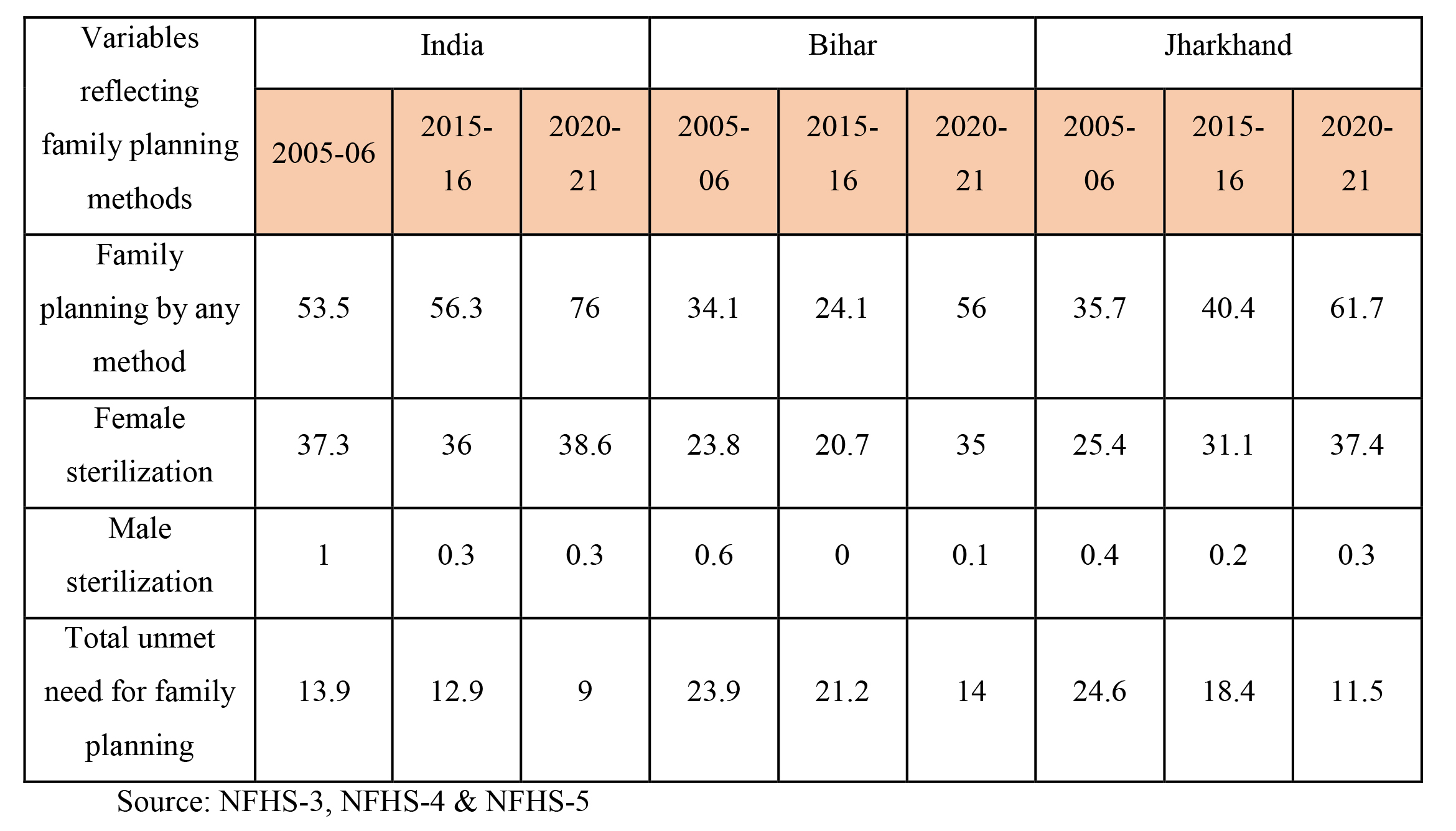
Family Planning Methods: Family planning methods are important in controlling the fertility rates. The performance of Bihar in adopting family planning techniques is not appreciable. During 2005-06, 34.1% currently married women practiced family planning and this percentage fell to 24.1 in 2015-16. However, the percentage increased to 56 during 2019-21. Similarly female sterilization in the state fell to 21% in 2015-16 from 24% in 2005-06 and then increased to 35% during 2019-21. Male sterilization was just 0.1% in 2019-21. Also unmet need for family planning fell to 14% from 21%. These data clearly explain high fertility rate in the state. Also it points out that government needs to have more concrete policies regarding family planning. On the other hand, performance of Jharkhand is quite impressive in this context. Family planning in the state improved to 61.7% from 40.4%. Female sterilization also improved to 37% from 31% and unmet need for family planning reduced to 11.5%. These data are well reflected in the fertility rate of 1.6% for the state. Table 1: Family Planning Methods during NFHS-3 & NFHS-4(figures are in percentages)
Maternal Health Care: In recent years, keeping in line with SDGs, Government of India has launched number of maternal and child health care programmes like JSY, JSSK etc. An analysis of National Family Health Survey data of various rounds clearly reflects an improvement in health standards in Bihar and Jharkhand. Further when a comparison with national figures is done we got some interesting results.
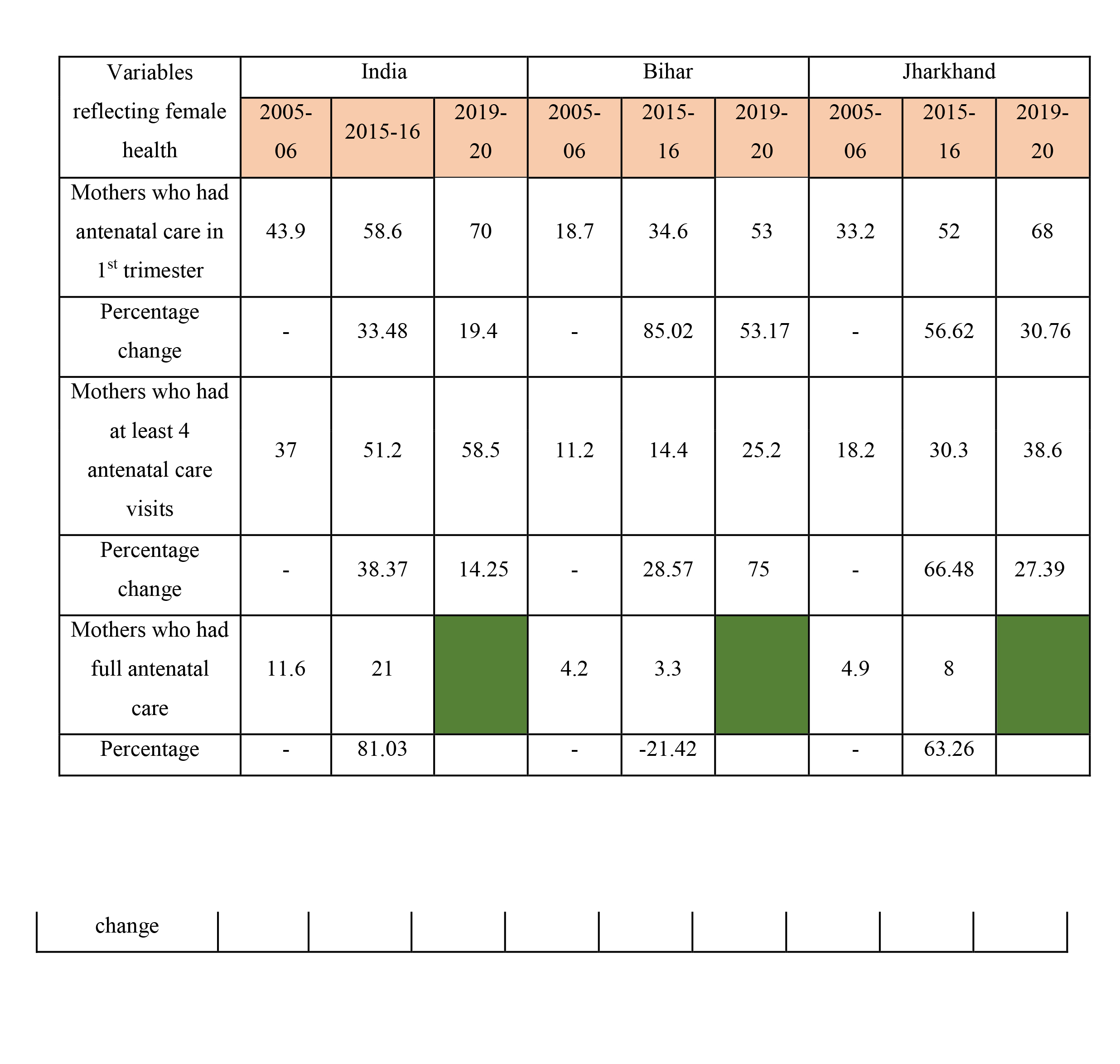
Antenatal Care: Proportion of mothers receiving antenatal care in 1st trimester has shown an increase both at national level and also at state level. However, the increase at state level is much higher than that at national level. Bihar has recorded highest percentage (53%) and the state of Jharkhand has also registered an impressive growth (37%) which is much higher than the figures at the national level (19%). Proportion of mothers receiving at least 4 antenatal care visits is much higher in Bihar (75%) as compared to both Bihar (28.57%) and all-India figure of 28.57%. On the other hand, data for mothers getting full antenatal care presents another picture (NFHS-3 & NFHS-4). At all-India level proportion of mothers receiving full antenatal care is quite high (81.03%). Jharkhand’s performance is quite impressive in this context (63.26%). However, proportion of mothers receiving full antenatal care has declined to 21.42% in Bihar which is a matter of concern for the government. The above analysis shows that performance of Jharkhand in providing antenatal care is better as compared to the performance of Bihar. Both these states need to be more focused in order to catch with the national figures.
Table 2: Antenatal Health Status during NFHS-3 to NFHS-5 (figures are in percentages)
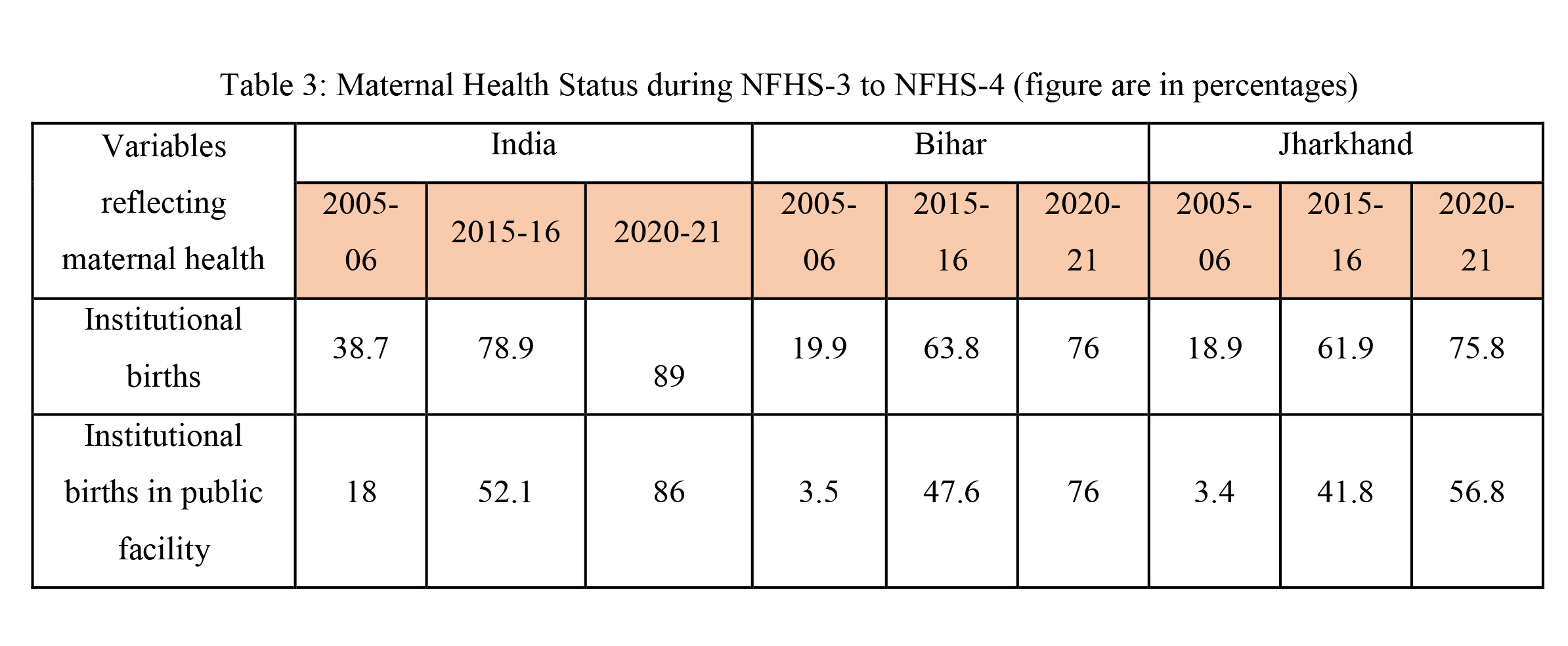
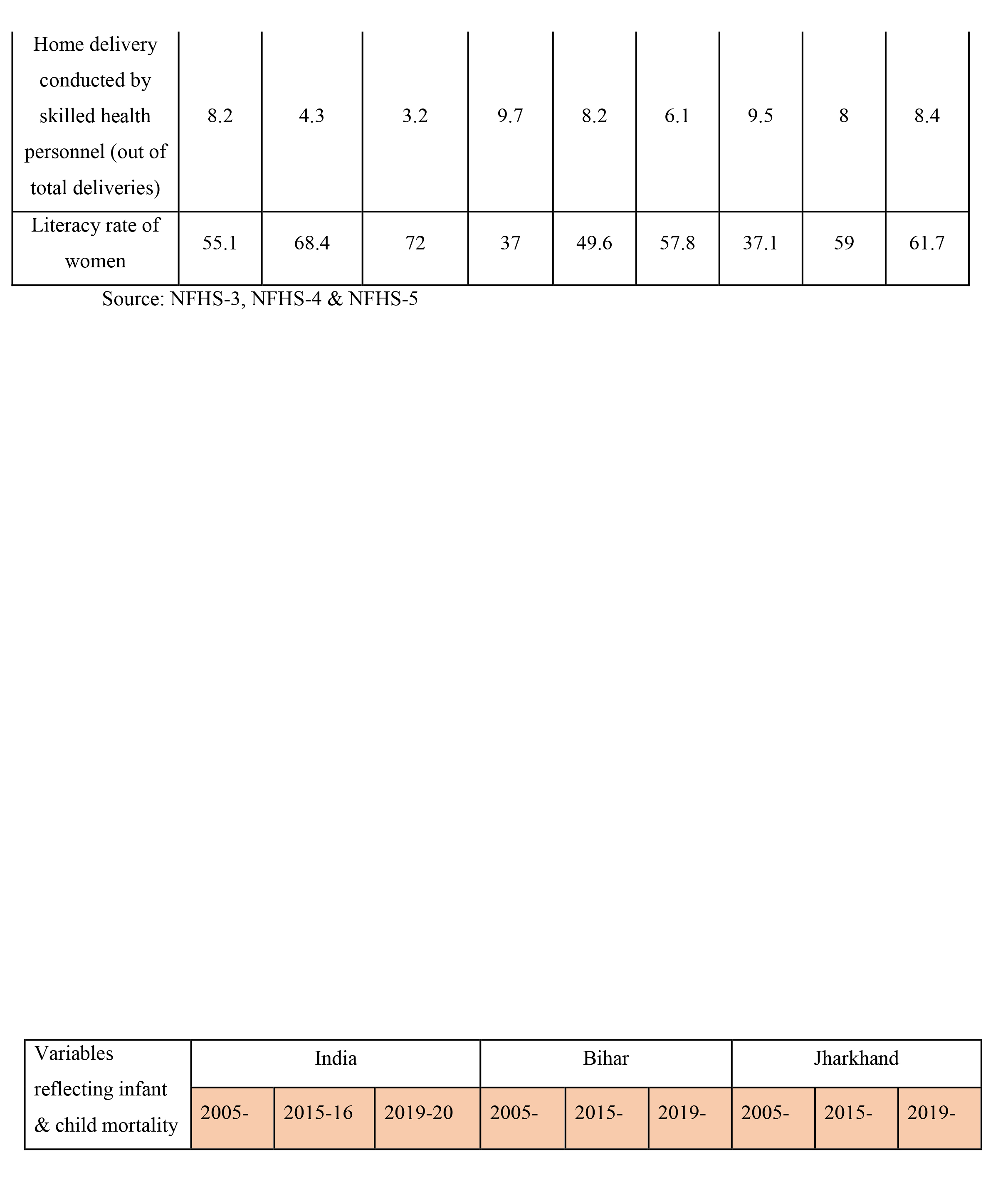
Institutional Delivery: Institutional delivery is an important component in determining maternal health and maternal mortality rate. Substantial improvement is being observed in this indicator. A percentage growth of more than 100% is observed in institutional births in both the states. It has increased from 20% (2005-06) to76% (2019-20) in Bihar and from 19% (2005-06) to 76% (2019-20) in Jharkhand. Institutional births in public facility have shown tremendous growth both at national level and at state level. In 2005-06 just 3.5% mothers had institutional birth in public facility in Bihar which has increased to 76% in 2019-20. Similarly in Jharkhand the increase has been to 57% from a mere 3.4%. At all-India level also now 86% mothers have used public facilities for deliveries. The proportion of females going for home delivery has reduced. This fall is more at national level as compared to state data. On one hand at all-India level 3.2% females had home delivery in 2019-20, the figures are 6.2% for Bihar and 8.4% for Jharkhand. The data also reveals substantial improvement in literacy rate of women. This clearly indicates that female literacy is an important determinant in determining maternal health. The improvement has been quite impressive in Jharkhand, the figures being 61.7% in 2019-20 as compared to Bihar (57.8%). However, both states need to put more effort in improving female literacy to catch with national figure of 72%.
Child Health & Nutrition
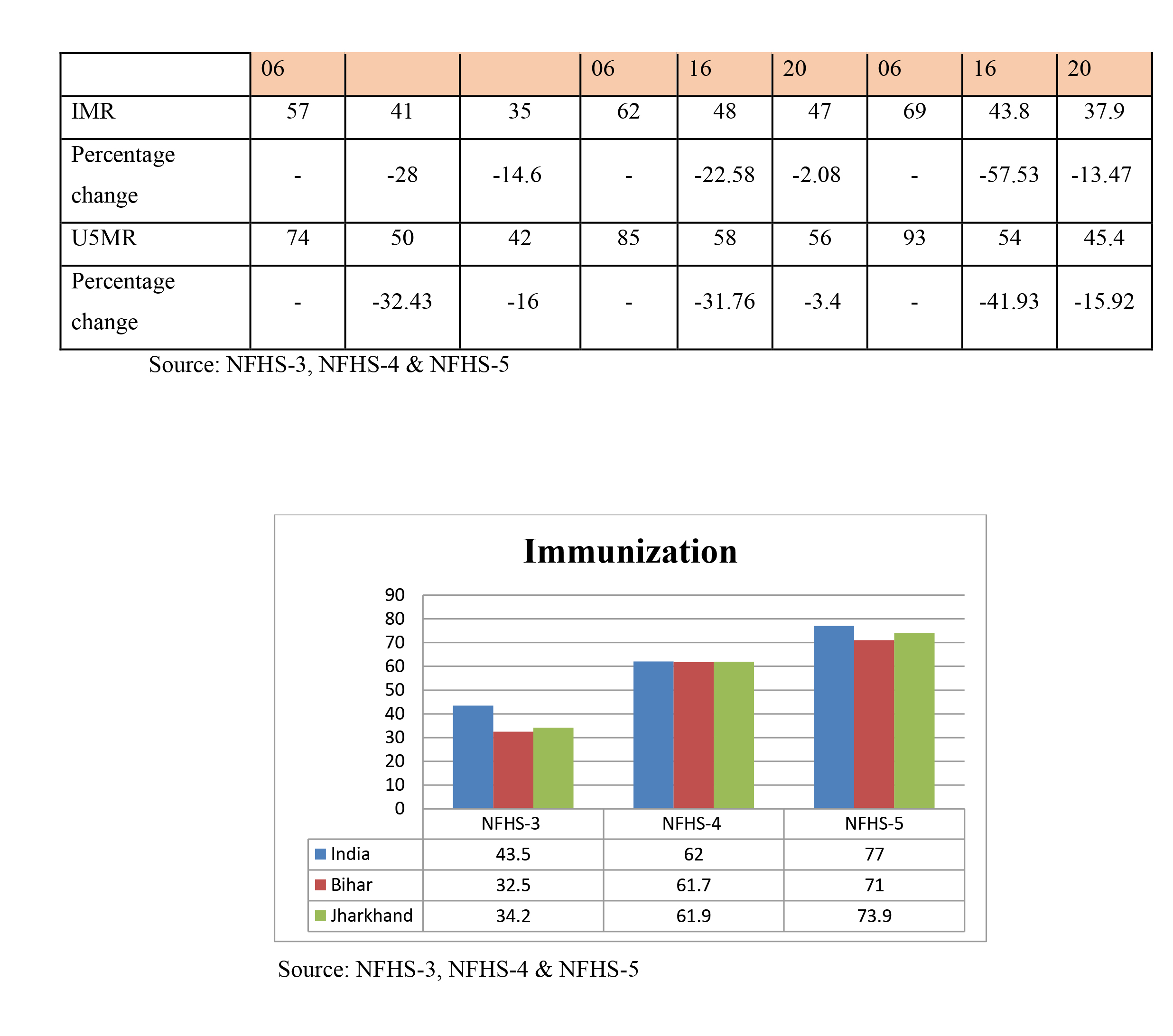
Mortality: Child health is well reflected in infant and child mortality figures. While IMR measures number of deaths of newborns under one year of age per 1000 live births, U5MR measures number of deaths of children under five years of age per 1000 live births. Improvement in both these data is observed over two survey periods. In 2005-06 IMR figures were 62 per 1000 in Bihar which has reduced to 48 per 1000 during 2015-16 and further 47 in 2019-20 indicating a reduction of over 22 percentage points from NFHS-3 to NFHS-4. Similarly, a 57% reduction is being observed for Jharkhand where during NFHS-3 to NFHS-4 and further a reduction of 37.9% was being observed during 2019-20. As far as U5MR figures are concerned, performance of Jharkhand has been very impressive. The state has registered a decline of around 53% over the two-survey period which is even higher than the national figure where a decline of 48 percentage points has been registered. U5MR figures reduced to 56 per 1000 in 2019-20 from 85 per 1000 during 2005-06. Bihar has also registered a decline of 34% over the decade. However more effort by the government is needed in infant and child health care to catch both with the national and with its immediate neighbour’s figures.
Table 4: IMR & U5MR during NFHS-3 to NFHS-5 (figures are in percentages)
Vaccinations: As per World Health Organization standards, full immunization of children aged 12-23 months is achieved when they receive one dose of BCG vaccine, three doses of DPT and polio vaccine and one dose of measles vaccine (EPW). An analysis of NFHS data shows that immunization coverage has improved since 2005-06. While during NFHS-3, total children having full immunization coverage was 43.5% at national level. Bihar and Jharkhand were having 32.5% and 34.2% coverage respectively. The two states have performed quite well (71% for Bihar and 74%) in this indicator as they are around national figures (77%) of full immunization coverage during 2019-20. Figure 2: Immunization during NFHS-3 to NFHS-5 (figures are in percentages)
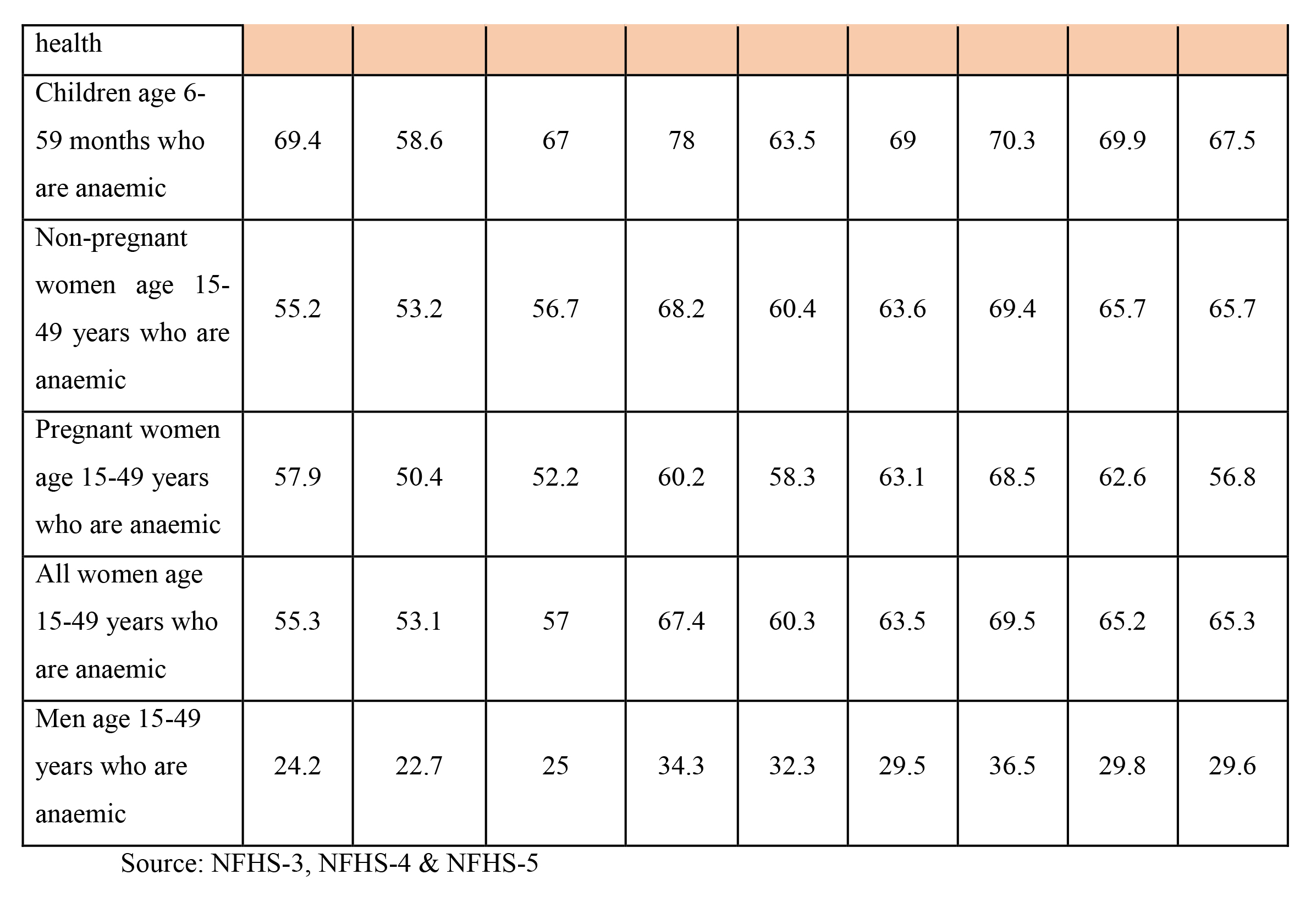
Anaemia: Anaemia is a medical issue which is characterized by low level of haemoglobin in blood. In developing countries this is a common problem found among children and also among adolescent girls and women of all age-groups. In this section extent of anaemia is being analysed for children, women and men. It can be found out from the preceding table that extent of anaemia is quite high among children up to 5 years both at state and at national level. In 2019-20, 67% children upto age 5 years were anaemic at the national level. In fact, a rise of 9 percentage points has been occurred since 2015-16. For Bihar, the figures are 69%, however, Jharkhand has shown an improvement in controlling the extent of anaemia among children. A fall of two percentage points is being observed for Jharkhand (from 69.9% in 2015-16 to 67.5% in 2019-20). This high extent of anaemia among children can be well correlated with high level of anaemia among pregnant women. In fact, anaemia happens to be problem with women in general. More than 50% of women in all age-groups are found anaemic in the nation. During NFHS-5, it was found out that the extent of anaemia in all age-groups is high in Jharkhand (65.8%) as compared to Bihar (63.5%) and all-India (57%) figures. However, some improvement in the data can be observed when compared from NFHS-3 and NFHS-4 data but the rate is very slow. On the contrary the data for men who are anaemic is comparatively low. These data reflect some important aspects. Firstly, anaemia is a common problem for the nation as a whole. The extent is high in females which shows neglect of female health. The reproductive cycle requires them to have nutrient rich food which seems completely missing as evident from the data. Poor health of females also causes poor and fragile health conditions for children. If the mother is anaemic certainly that will pass on to the child. These figures are of great concern for the government. If maternal and child health is to be prioritised them the initial step should be of controlling anaemia and providing adequate health supplements to pregnant women.

Table 5: Anaemia in Mothers and Children during NFHS-3 & NFHS-4 (figures are in percentages)
Breastfeeding: Breastfeeding is an important element which determines both child and maternal health. Percentage of children who were breastfed within one hour of birth has increased substantially. In past one decade percentage of children who were breastfed within one hour of birth increased to 30% in Bihar. Similar increase is being observed in Jharkhand and at national level. The figures for children under age 6 months who were exclusively breastfed are highest in Jharkhand (76%). Substantial improvement has been registered in Bihar where the figures have increased from 28% during 2005-06 to 59% during 2019-20.
Table 6: Breastfeeding Status during NFHS-3 to NFHS-5 (figures are in percentages)
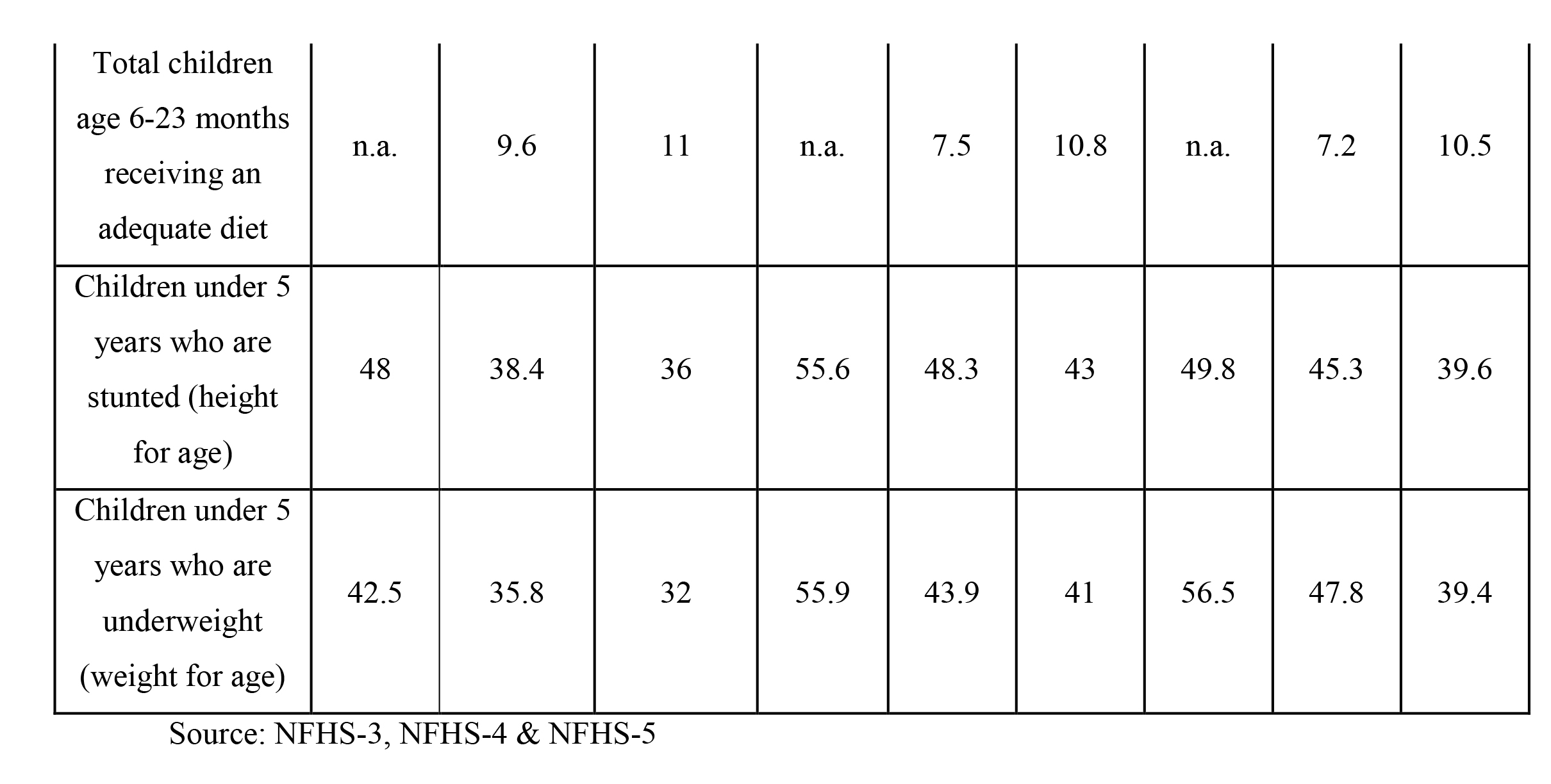
Malnutrition in Children: The nutritional status of children in the nation appears to be a matter of great concern as reflected in the health survey data. Malnutrition in the present analysis is calculated by measuring children receiving adequate diet, height and weight of children up to 5 years of age. Total children up to 2 years of age receiving an adequate diet is quite low both for the state and for the nation. The figures are almost same for Bihar (10.8%) and Jharkhand (10.5%). Even at national level only 11% children have received adequate diet upto 2 years of age. A percentage decline in the figures for children under 5 years who are stunted and underweight has been observed both at the national and at the state level. A percentage decline ranging between 6 to 10 is observed, however the figures are still high in Bihar and Jharkhand. Thus, it can be seen that the extent of malnutrition is quite high in Bihar and Jharkhand.
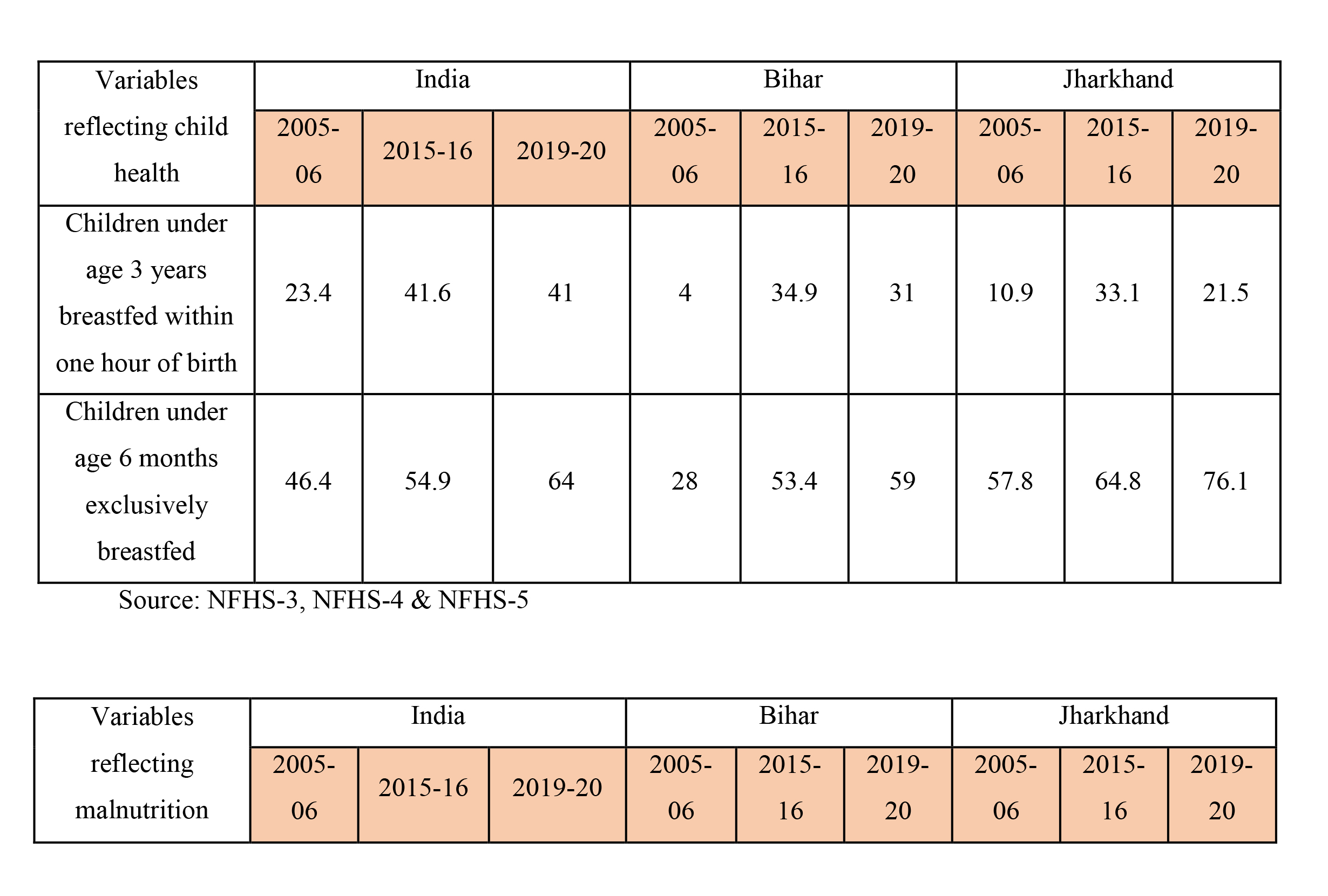
Table 7: Malnutrition during NFHS-3 to NFHS-5 (figures are in percentages)
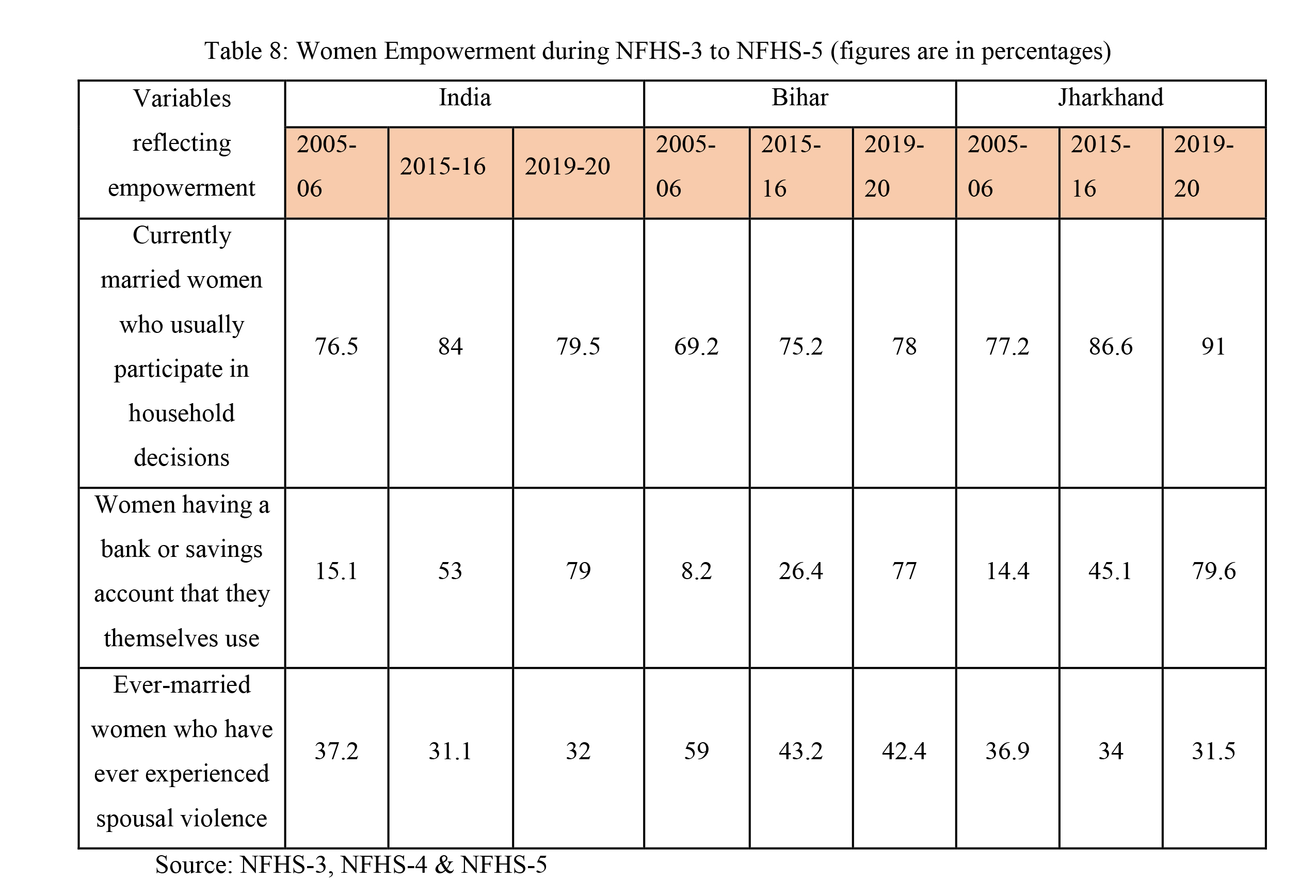
Empowerment of Women: Factors like women having a bank or savings account and females participating in household decision making are considered in the present analysis as an indicator of women empowerment. Social status of females has improved as indicated by the survey data. Percentage of currently married women who usually participate in household decision is around 80% at national level. In Bihar (78%) and Jharkhand (91%) also more than three-fourth of married women participate in household decisions. Sharp increase of 64 percentage points in women having a bank or savings account is registered at national level (from 2005-06 to 2019-20). Similar trend is being observed in Jharkhand (66%) and Bihar (69%). Cases of spousal violence among ever-married women have also declined. Bihar has registered a decline of 16.6% which is substantially higher than the decline in Jharkhand (5.9%) and all-India figure (5.2%) [from 2005-06 to 2019-20]. Thus it can be said that over a decade, financial participation of females has increased which reflects financial inclusion. Moreover, between the two states social status of women in Jharkhand is found comparatively better than that in Bihar.
Health Expenditure
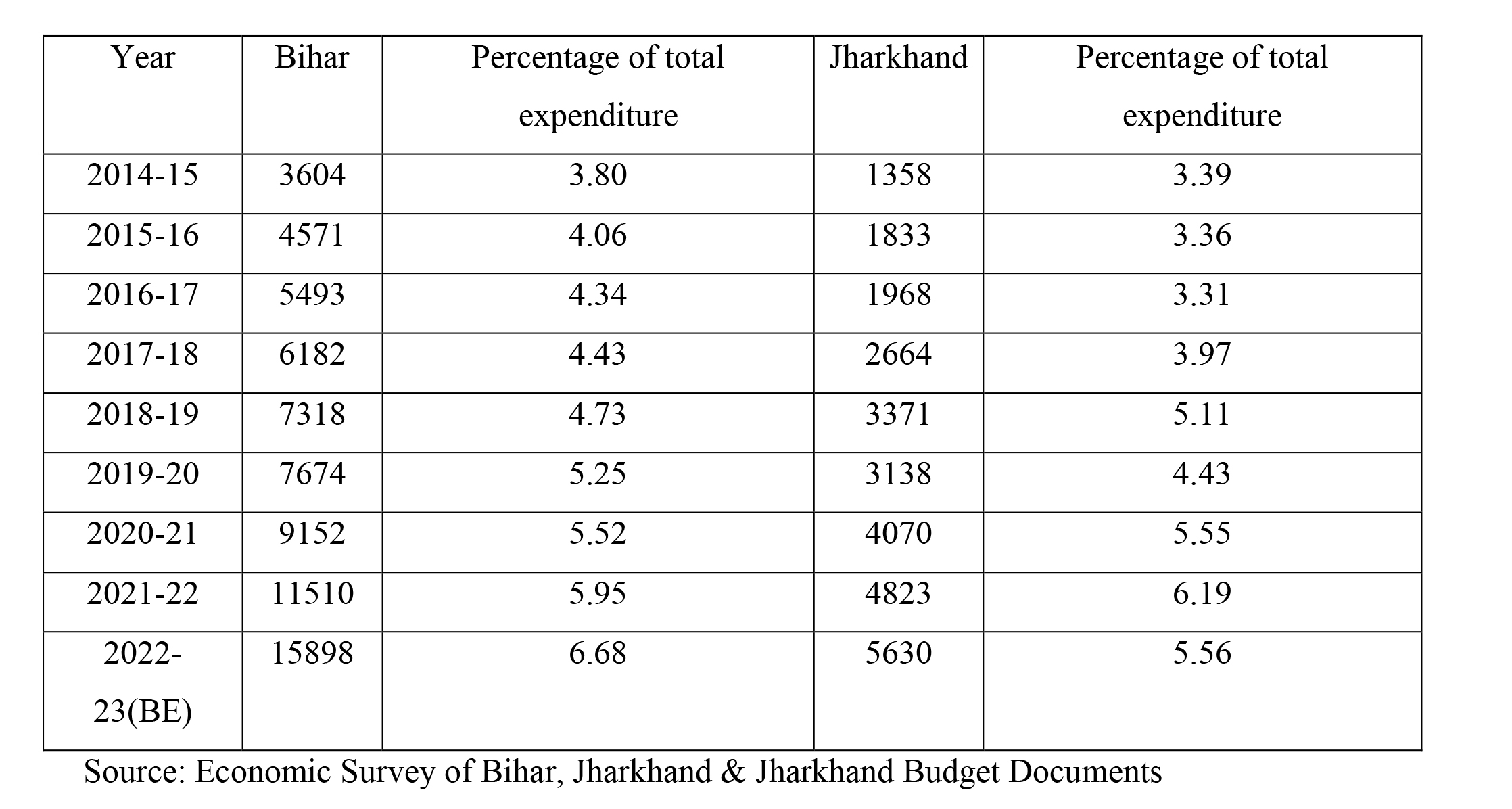
This section presents government expenditure on health in Bihar and Jharkhand. Government expenditure on health is essential to improve the maternal and child health conditions. As can be seen (Table 9) expenditure on health in Bihar has constantly increased both in absolute and in percentage terms. In absolute terms it seems that health expenditure in Bihar is greater than that in Jharkhand. However, as a percentage of total expenditure on social services both the states are spending more or less the same amount on health and family welfare activities. The maternal and child health indicator varies in the two states which show variations in execution of the expenditure done on health services.
Table 9: Health Expenditure in Bihar and Jharkhand (crores)
Concluding Remarks and Policy Recommendations
The above analysis indicates that maternal and child health conditions are comparatively better in Jharkhand as compared to Bihar. However both states lack in matching the figures with all-India level. Sharp improvement in health indicators over the survey period have been found out in Bihar which shows clear vision of Government in improving maternal and child health status in the state. Jharkhand has also registered an impressive positive change in health indicators over the decade. Anaemia and malnutrition has been observed as a serious concern and more concrete efforts are needed in this direction. Hence it can be said proper execution of all government programmes related with maternal and child health is required to get the desired results.
REFERENCES